
Results and discussion: Macrolevel trends in use of services provided by health workers
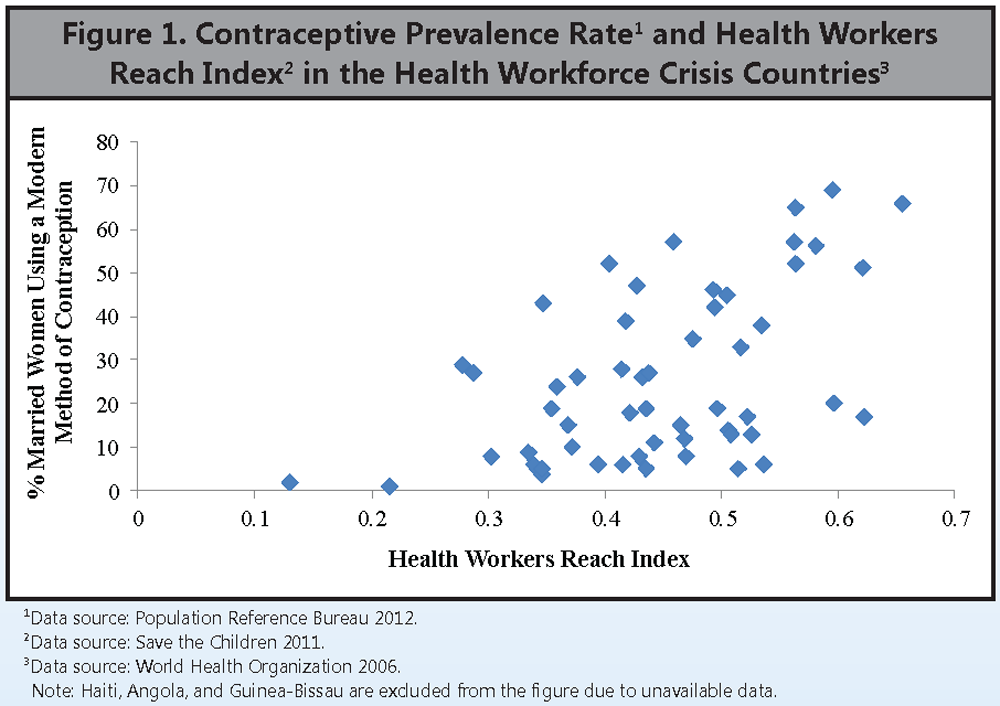
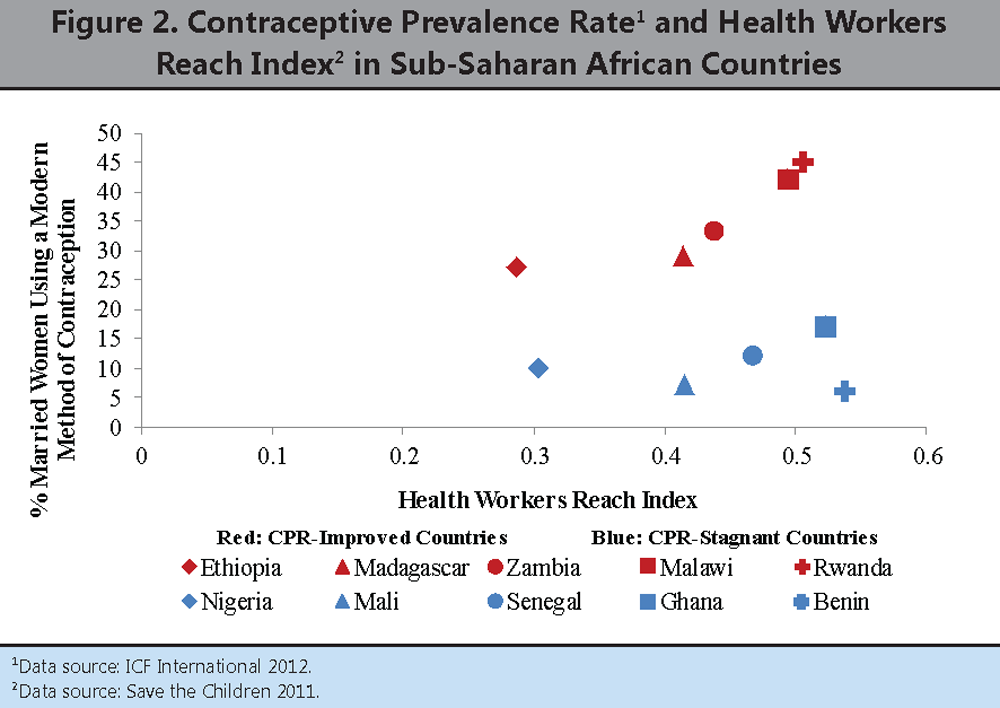
 Given that health workers are needed to provide contraception, one might expect countries with higher HWRI scores to have higher CPRs. As shown in Figure 1, this is the case overall. As HWRI scores increase among the health workforce crisis countries, the CPR also tends to increase. However, it is also apparent that there are countries with almost identical HWRI scores but very different CPRs. This finding is illustrated more vividly in Figure 2, which shows the HWRI scores and CPR values for the 10 sub-Saharan African countries selected for this analysis. Unexpectedly, the HWRI scores for the CPR-improved countries cover the same range as do the scores for the CPR-stagnant countries. In fact, for every country in the CPR-improved grouping, there is a country in the CPR-stagnant grouping with approximately the same HWRI score.
Given that health workers are needed to provide contraception, one might expect countries with higher HWRI scores to have higher CPRs. As shown in Figure 1, this is the case overall. As HWRI scores increase among the health workforce crisis countries, the CPR also tends to increase. However, it is also apparent that there are countries with almost identical HWRI scores but very different CPRs. This finding is illustrated more vividly in Figure 2, which shows the HWRI scores and CPR values for the 10 sub-Saharan African countries selected for this analysis. Unexpectedly, the HWRI scores for the CPR-improved countries cover the same range as do the scores for the CPR-stagnant countries. In fact, for every country in the CPR-improved grouping, there is a country in the CPR-stagnant grouping with approximately the same HWRI score.
{kind=link}
{kind=link}
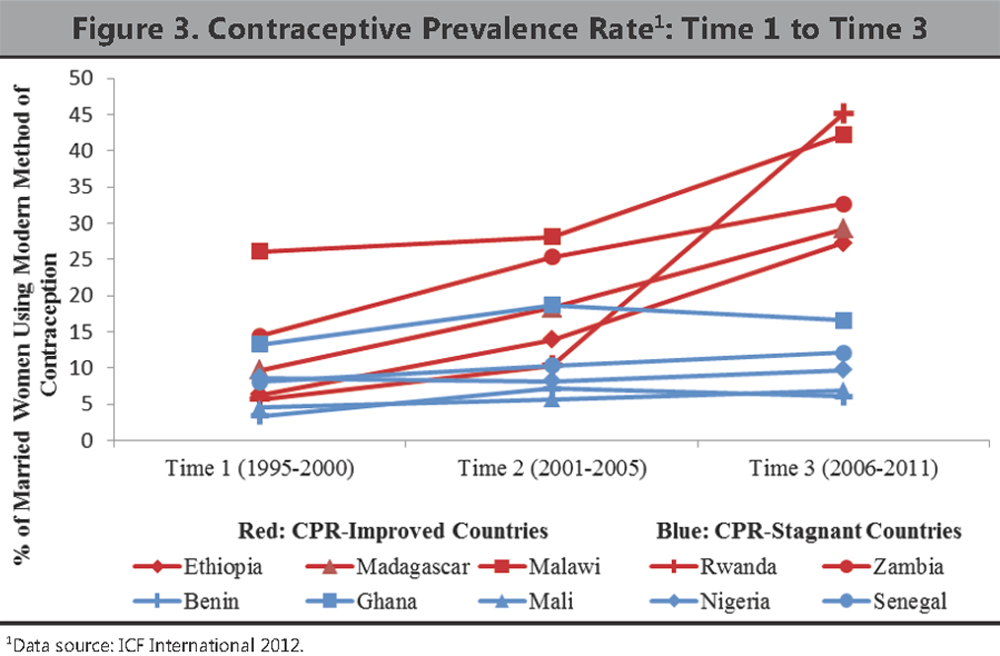
To further explore this finding, we examined the two subcomponents of the HWRI derived from the DHS (SBA and DPT3) with a focus on trends in the values of these indicators for the two groupings of countries. Our intent was to ascertain if levels and trends in these two measures of health worker access were moving in the same or different direction as the CPRs: 1) for individual countries; and 2) for each grouping of countries over the 10–15 year time period. As stated previously, due to poor data quality issues and the fact that the health worker density ratio is not a DHS indicator that can be associated with a definitive time period and systematically analyzed over time, the health worker density ratio was not included in this subanalysis.
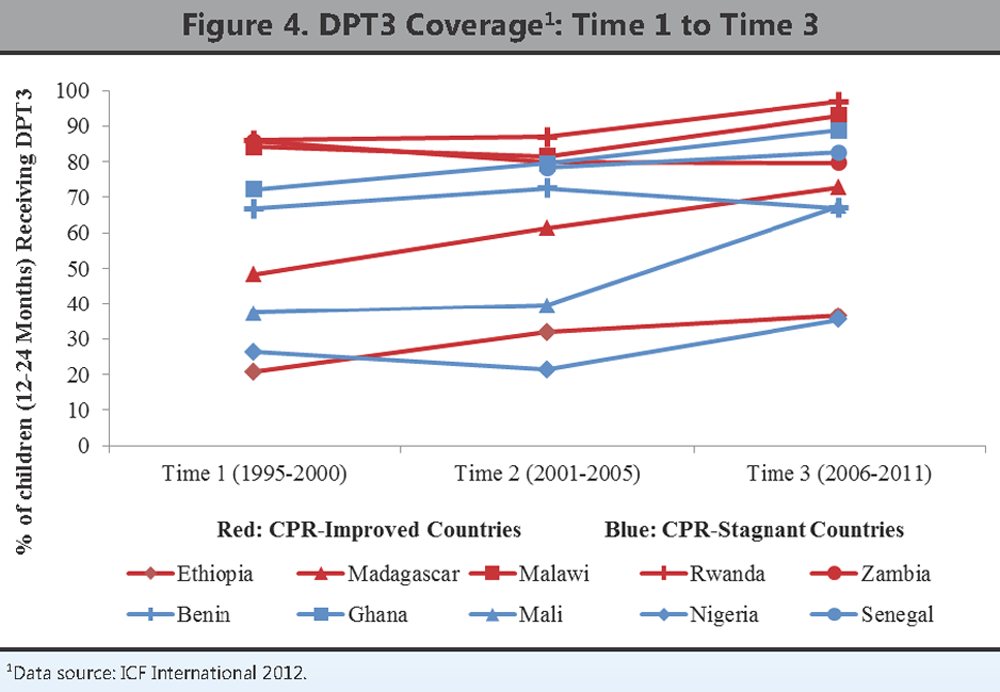
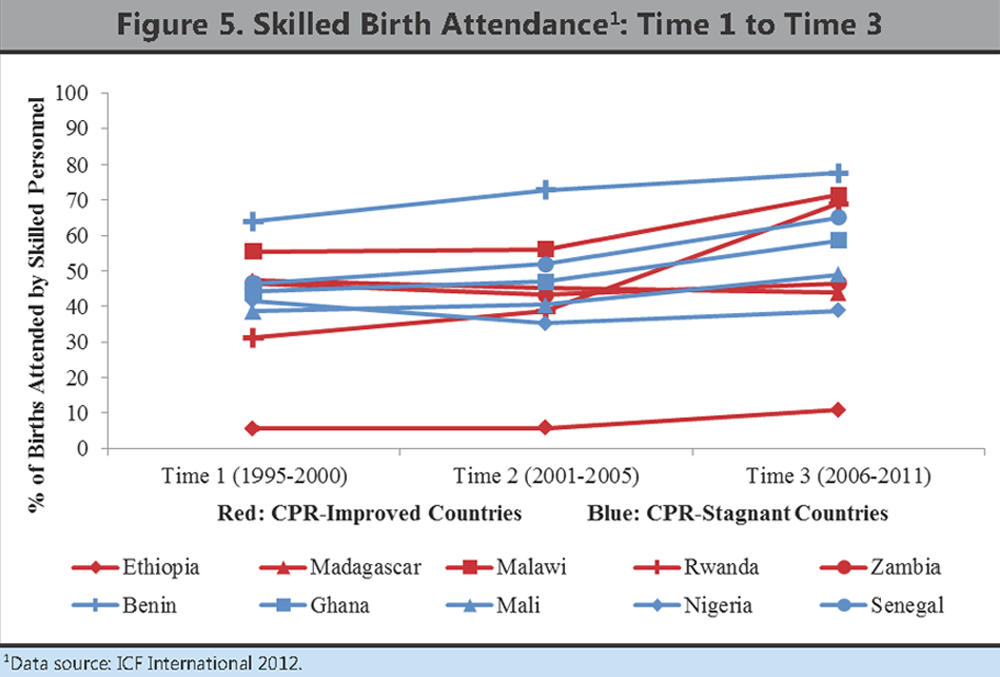
Skilled birth attendance and receipt of DPT3 require access to a health worker, as does the use of most methods of modern contraception. Yet Figure 3, Figure 4, and Figure 5 reveal that the CPR-improved countries did not necessarily experience greater percentage point increases in or higher levels of skilled birth attendance and DPT3 coverage than the CPR-stagnant countries over the study period. In fact, with respect to the most recent DHS values for these two indicators, many of the CPR-stagnant countries have been able to maintain or achieve similar levels of SBA and DPT3 coverage as have the CPR-improved countries (see appendix). Furthermore, in some instances, the CPR-stagnant countries have been able to establish better population coverage for specific health services. For example, Benin, a CPR-stagnant country, has achieved the highest national skilled birth attendance rate (78%) among all 10 countries for the most recent time period. Both Ghana and Senegal, CPR-stagnant countries, have higher national DPT3 immunization coverage (89% and 83%, respectively) in the most recent time period than three CPR-improved countries—Ethiopia (37%), Madagascar (73%), and Zambia (80%). Among the 10 countries, Rwanda, a CPR-improved country, achieved the highest percentage point increase in SBA coverage (38) over the study period; however, Mali, a CPR-stagnant country, achieved the highest percentage point increase in DPT3 coverage (30).
{kind=link}
{kind=link}
{kind=link}
One implication of these findings is that how health workers are trained, distributed, and supported may be as important as how many health workers are available at the national level. CPR-improved countries may have made different decisions than CPR-stagnant countries about how to develop, deploy, and support their family planning health workforce, just as some CPR-stagnant countries with improved SBA and DPT3 rates may have made different decisions related to their maternal and child health workforces. To further explore this question, we examined differences in urban/rural contraceptive use, method type, and source of method among the 10 countries using DHS data.