
Results and discussion: Contraceptive method type
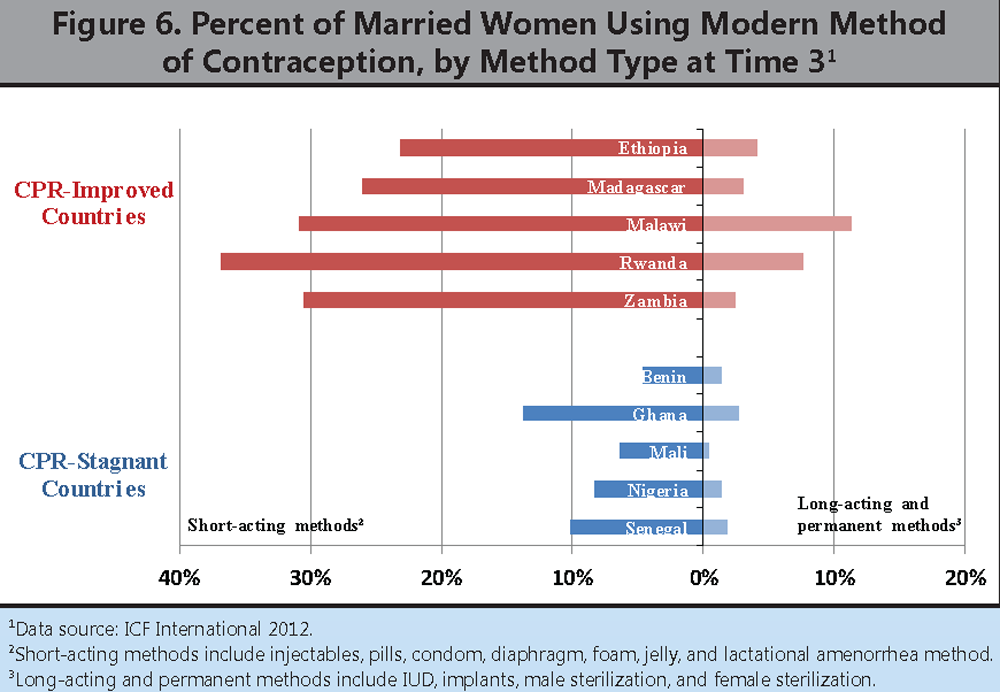
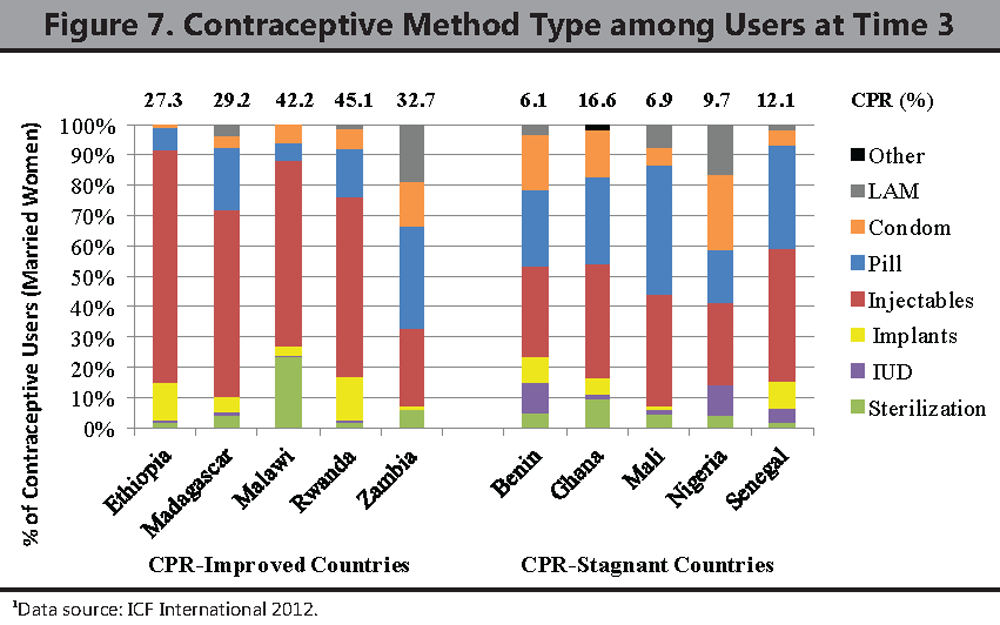
 Short-acting methods (injectables, pills, condoms, diaphragm, foam, jelly, and lactational amenorrhea method [LAM]) are by far the most commonly used methods in both CPR-improved and CPR-stagnant countries at time 3 (Table 1 and Figure 6). Injectable contraception is the most common method of contraception in eight out of the 10 countries, whereas the pill is the most common method of contraception in Mali and Zambia (Figure 7). Injectable contraception is the method of choice for 50% of all users in four out of the five CPR-improved countries. None of the CPR-stagnant countries has any method that makes up more than 50% of users, and married women in CPR-stagnant countries use injectable contraception less frequently (27%–43% of users) than do those in CPR-improved countries. Also of note, the method mix is more varied in the CPR-stagnant countries, with higher proportions of users adopting methods such as pills, condoms, and LAM that traditionally require fewer highly skilled providers or no provider at all.
Short-acting methods (injectables, pills, condoms, diaphragm, foam, jelly, and lactational amenorrhea method [LAM]) are by far the most commonly used methods in both CPR-improved and CPR-stagnant countries at time 3 (Table 1 and Figure 6). Injectable contraception is the most common method of contraception in eight out of the 10 countries, whereas the pill is the most common method of contraception in Mali and Zambia (Figure 7). Injectable contraception is the method of choice for 50% of all users in four out of the five CPR-improved countries. None of the CPR-stagnant countries has any method that makes up more than 50% of users, and married women in CPR-stagnant countries use injectable contraception less frequently (27%–43% of users) than do those in CPR-improved countries. Also of note, the method mix is more varied in the CPR-stagnant countries, with higher proportions of users adopting methods such as pills, condoms, and LAM that traditionally require fewer highly skilled providers or no provider at all.
{kind=link}
{kind=link}
Long-acting and permanent methods (LAPM) include male and female sterilization, IUDs, and implants. Administration of LAPM typically requires access to more highly skilled health workers, such as doctors, nurses, or midwives. Steady increases in urban and rural LAPM use are observed in several of the CPR-improved countries, except for Madagascar and Zambia, which experienced only slight changes in LAPM use over the 10–15 year period (Table 1). At time point 1 (1995–2000), the percentage of married women reporting use of an LAPM in Ethiopia, Malawi, and Rwanda was 0.4%, 5%, and 1% respectively. Over the next 10–15 years, use had risen to 4.2%, 11.4%, and 7.6% respectively. On the other hand, use of LAPM at the most recent time point is less than 3% among married women in all five of the CPR-stagnant countries. In fact, several of the CPR-stagnant countries show declines in LAPM use over the 10–15 year time period, especially in urban areas. For example, 2.3% of married women in Senegal reported use of a LAPM in 1997 but only 1.9% did so in 2011.
- Health workforce determinants at play? Ensuring that populations have equitable access to a range of contraceptive methods requires that barriers related to which cadres can provide family planning methods be reduced by redefining legal scopes of practices, and that health workers who are then legally able to provide different types of contraception are appropriately trained, distributed, and retained throughout the country according to population needs. Since the type of health worker needed to provide contraception varies by method, the differentials in contraceptive use by method between countries may reflect, in part, differentials in access to specific cadres of trained health workers, especially in rural and underserved periurban areas. Use of certain types of methods may also partly reflect differences in health worker training, qualifications, and preferences, even within a given cadre.