
Appendix: Quantifying Public Sector Absenteeism
 In countries facing a health worker shortage, quantitative research shows high rates of absenteeism. Absence rates are calculated as the number of person days lost in a given time period over the total number of workable person days in that period. For the purposes of observation, it is the fraction of health workers contracted for service but not on site during the period of observation.
In countries facing a health worker shortage, quantitative research shows high rates of absenteeism. Absence rates are calculated as the number of person days lost in a given time period over the total number of workable person days in that period. For the purposes of observation, it is the fraction of health workers contracted for service but not on site during the period of observation.
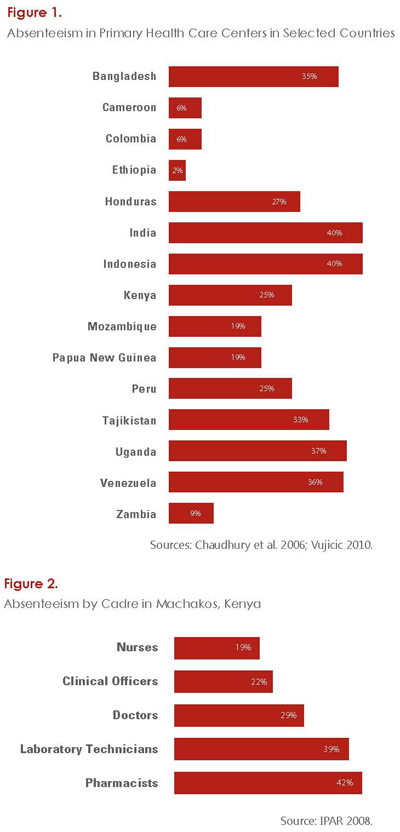
To the extent possible, it is helpful to examine the heterogeneity of absence rates (see Figure 1). Chaudhury et al.’s (2006) multicountry study revealed that smaller health facilities, higher-level cadres of health workers, and facilities serving poorer communities were all positively correlated with greater rates of absenteeism. In addition, men were more likely than women to be absent, and cadres more able to make money in private practice were more likely to be absent.
In Kenya, an absenteeism study disaggregated by cadre demonstrated that pharmacists and lab technicians were twice as likely to be absent than nurses; pharmacists gain substantial financial rewards through private-sector opportunities (IPAR 2008) (see Figure 2). In Bangladesh, doctors recorded disproportionately higher rates of absenteeism (42%) compared to their colleagues from other cadres (<27%) (Chaudhury and Hammer 2003).
The most common characteristics for absenteeism are when the health worker:
- Is a higher-level cadre/has higher authority (e.g., doctors and managers)
- Is male
- Has greater opportunity to earn money in private practice (e.g., doctors, pharmacists, lab technicians)
- Is posted in a poor, remote or rural community
- Is posted at a lower-level health facility
- Was recruited to a post without being informed of the post’s geographical location.